Hospice Caps
To ensure that the cost of hospice care does not exceed the cost of conventional care, CMS established two annual caps (or limits) on hospice payments. The period (or cap year) is normally a 12-month period from October 1 to September 30. (Reference: CMS Pub. 100-02, Medicare Benefit Policy Manual, Chapter 9 (PDF))
Limit 1: Inpatient Day Limitation
Inpatient days (general inpatient and inpatient respite care) are not to exceed 20 percent of the total Medicare days. If inpatient days exceed 20 percent of total days, the payment for those days is reduced to the Routine Home Care rate.
Limit 2: Aggregate Cap on Overall Reimbursement
Medicare payments are subject to an aggregate cap for each cap year. The hospice's aggregate cap is calculated by multiplying the statutory cap amount (national rate) by the count of Medicare beneficiaries (specific to hospice and year). In the calculation, Medicare payments are compared to the aggregate cap. Payments more than the cap are overpayments and must be refunded to the Medicare program.

Statutory Cap Amount
The statutory cap amount, which is the same for all hospices, is updated each year by CMS.
|
Cap Year End |
Statutory Cap Amount |
|---|---|
|
9/30/22 |
$31,297.61 |
|
9/30/23 |
$32,486.92 |
Note: Newly certified hospices with an initial cap period longer than 12-months will use a weighted cap amount as computed by the MAC.
Beneficiary Count
The counting of Medicare beneficiaries is a complex calculation. Fortunately, the PS&R System captures the claims data and offers the needed reports.
The two methods of counting Medicare beneficiaries are Proportional and Streamlined.
a) Proportional Method (applies to most hospices)
Under the Proportional Method, a beneficiary receives a "lifetime" count of "1." A portion of this count of “1” is allocated to each year and to each hospice that provides services.

The PS&R System continuously updates with claims data. When a beneficiary receives additional hospice care, allocations in earlier years are reduced (the “lifetime” count of “1” is allocated across a larger service history).
The sum of all beneficiary allocations (at one hospice — for one cap year) is the beneficiary count for that hospice.
In the following example, please note how hospice services in prior and later years (and from other hospices) affects Hospice A’s 2022 beneficiary count. (Years cited refer to cap years.)
Hospice A had three patients in 2022.
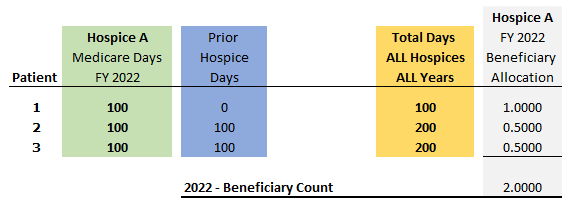
Impact of Prior Hospice Care
Patients 1, 2 and 3 each received 100 days of care from Hospice A.
- Patient 1: allocation = 1.00 (only care is from Hospice A in 2022)
- Patient 2: allocation = .50 (100 days of care from Hospice A in 2021)
- Patient 3: allocation = .50 (100 days of care from Hospice B in 2019)
Impact of Later Hospice Care on the 2022 Beneficiary Count
- Patient 1: no additional hospice care
- Patient 2: 200 days of care in 2023 from Hospice A
- Patient 3: 200 days of care in 2025 from Hospice C
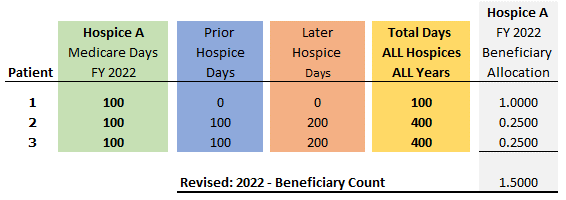
After revising for later services, Hospice A’s 2022 Beneficiary Count decreased by 25 percent (from 2.0 to 1.5), which reduced the aggregate cap by 25 perecent. The revised aggregate cap is compared to the Medicare payments to determine if there is an overpayment.
See Proportional Method — Case Studies (PDF) for additional examples of the beneficiary allocation under the Proportional Method.
b) Streamlined Method (only available if elected in 2012)
If a beneficiary only receives care from a single hospice, the beneficiary is counted in the year hospice care is elected (and not counted in subsequent years). If care is received from more than one hospice, then the portion of the patient's stay is calculated as under the Proportional Method.
Self-Determined Hospice Cap (SDHC) Report
Hospices must submit a Self-Determined Hospice Cap (SDHC) Report each year. This SDHC report is due no later than five months after the end of the cap year (end of February).
Please see Hospice Cap Self-Reporting for forms and instructions.
Cap Reviews and Revisions made by the MAC
Each year Palmetto GBA performs a review of the hospice cap and incorporates any SDHC overpayment. This review also evaluates prior years to determine if there have been material changes (such as a change in the beneficiary count).
After completing the review, a notice of “Inpatient Day Limitation and Hospice Cap Amount” is issued. If material changes are noted in prior year reviews, the prior year determination(s) is reopened and revised. CMS requires contractors to review the three prior years as part of the current year review. Of note, if a hospice initially exceeded (or was close to exceeding) the aggregate cap, a revised determinations for that year may result in an additional overpayment.
Tool — Hospice Cap/Inpatient Day Limitation Estimator
To assist in monitoring the aggregate cap and inpatient day limitation, the following tool is available: Hospice Cap & Inpatient Day Limit Calculator
This tool allows one to enter projected data to estimate where the hospice is in relation to the limits.